

Shoulder pain and dysfunction can have a variety of root causes. Chiropractors will directly or indirectly address shoulder problems since a large percentage are related to poor function and alignment of the cervical spine and upper thoracic spine preventing normal alignment of the shoulder girdle. However in this particular blog I want to talk about the more intrinsic presentation of shoulder pain and dysfunction, called shoulder impingement syndrome.
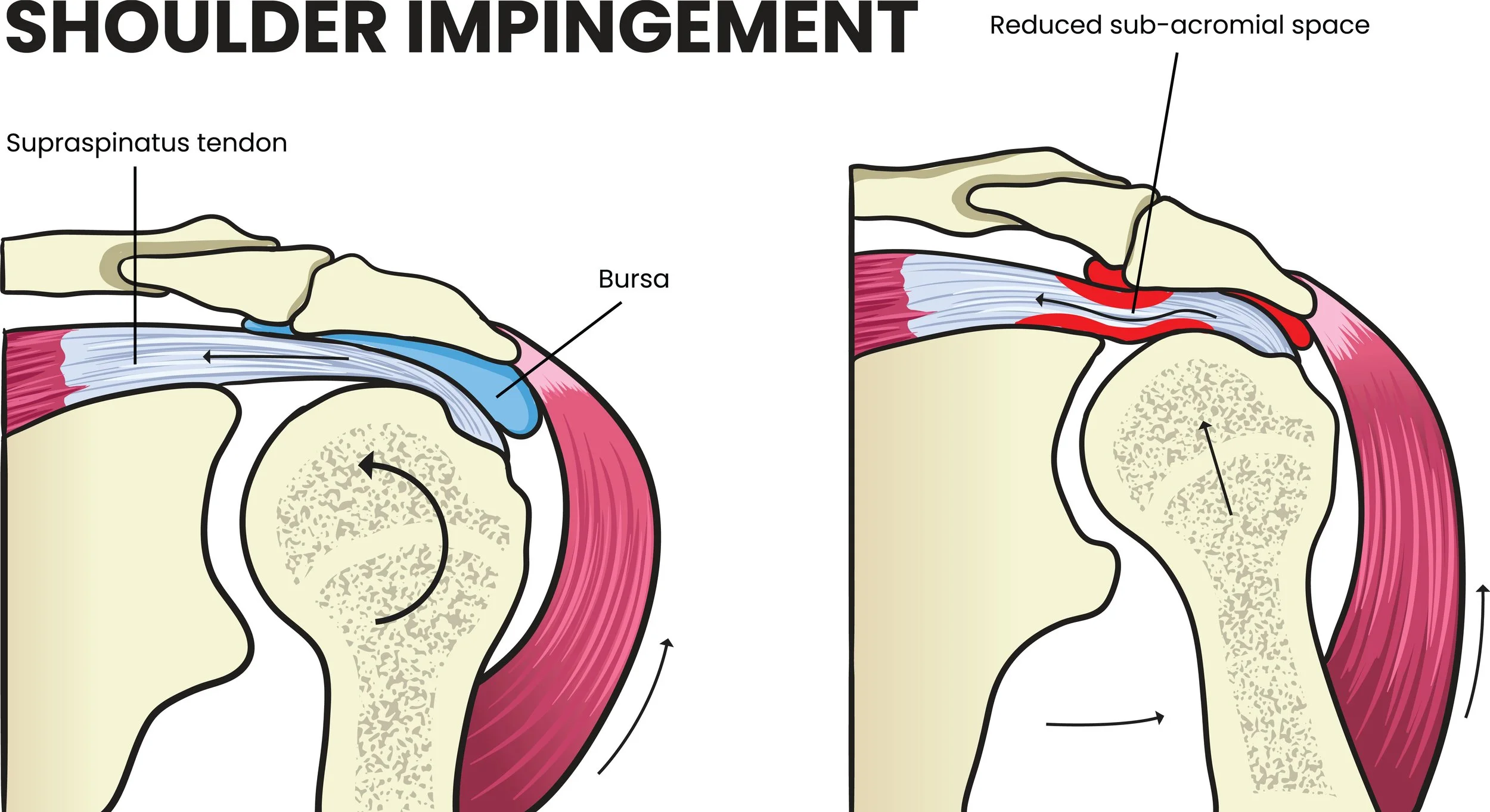
Shoulder impingement syndrome is actually a bit of a broader umbrella itself. In a nutshell, it describes a problem whereby the space above the ball of the head of the humerus and the bony bridge of the a acromioclavicular joint is narrowed, causing a pinching of the structures located in between, mostly some of the rotator cuff tendons and the bursa.
Shoulder impingement syndrome can fall into 2 categories, which sometimes overlap:
– static impingement syndrome describes a more or less permanent narrowing that is not affected by the movement and position of the arm. This happens when there is for example a bony outgrowth on the inferior aspect of the acromioclavicular joint, or some calcification of the tendon. The impingement will be the same regardless of the position of the arm. Those tend to be more difficult to resolve conservatively, since there are fewer ways to impact the problem. Thankfully it's a minority of the shoulder impingement presentations.
– Dynamic impingement syndrome describes an impingement that is the variable based on the position and movement of the arm. The vast majority of impingement syndromes are in the anterior aspect of the shoulder, sometimes lateral, and infrequently posterior. The main reason for the anterior dominance have to do with modern humans tendency to have very dominant anterior shoulder muscles pulling them in a rounded forward shoulder position, as well as the fact that the shape of the acromioclavicular joint tend to slope downward in the front of the shoulder, thereby predisposing more easily to impingement in the front.
Presentation of dynamic impingement syndrome often is anterior shoulder pain, sometimes radiating down the arm, when the arm is repetitively moving above the head or to decide, especially if additional weight is held, more pain when the shoulders slumped forward, or if this pressure to the anterior arm such as when sleeping on that side. Shoulder impingement syndrome is often found in combination with other shoulder problems such as acromioclavicular bony spurs, anterior frozen shoulder.
Resolving a shoulder impingement syndrome requires to look at all the modifiable factors that can be corrected to improve the clearance of the humeral head in relationship to the acromion especially when the arm is lifted forward or to the side:
– alignment of the neck and upper back in relationship to the shoulder blades. Anterior neck postures, rounded mid back and shoulder blade well-positioned the humeral head forward, in an already narrow subacromial space.
– Muscular balance between the front and back of the shoulder, which often goes with the anterior neck and upper back posture. This will require some manual release of the anterior contracted musculature and some passive as well as active retraining of the posterior shoulder stabilizers.
– Chronic scar tissue in the bursa, rotator cuff tendons, and anterior joint capsules. Those can fixate the head of the humerus superior and anterior, effectively narrowing the subacromial space with little to no margin during arm flexion and abduction. Manual adjustments of the humeral head as well as very specific soft tissues scar releases important to resolve this.
– Scar tissue and myofascial adhesions in the muscle group known as "humeral depressors", which are deep axillary muscles, in charge of pulling the head of the humerus down during arm flexion and abduction in order to create a little more space for the rest of the rotator cuff tendons. I find that to be often the missing part of the treatment plan to resolve long-standing shoulder impingement syndrome when people have already been working with physical rehab.
– Revisiting some of the patient's chronic triggers from the activities: sleeping position on the side without adequate support of the cervical spine can set up a cycle of chronic recurrent shoulder pain. Technology has been a huge problem, especially as computer use requires less keyboarding and more computer mouse usage, with the arm chronically rotating anterior. Ergonomic modification of the placement and type of computer mouse can be really helpful.