It's a question that comes up periodically and since there is no easy answer that I can give to patient during a routine appointment slot, I decided to put my thoughts in writing so I can refer patients to it as a conversation starter.
The groin is a small piece of the body's real estate, that we tend to think of as private, but that can really control your life if it starts acting up.
It's a body area that is the intersection of several structures that can be pain producing, and you need a little bit of attentive detective work to determine the source of the problem.
The main structures that can be involved in producing groin pain:
– referred pain from the middle lumbar area, especially L2 and L3 segments. These would be things like a lumbar disc herniation causing pain to radiate along these dermatomes, or significant bony spurs. The lower lumbar segments such as L4 5 and L5 S1 definitely take the lines shares in terms of referred this pain, so that sometimes we tend to forget that mid lumbar areas can also be a source of referred pain. Patients with groin pain referred from these mid lumbar segments tend to have pain that is aggravated by lumbar movement.
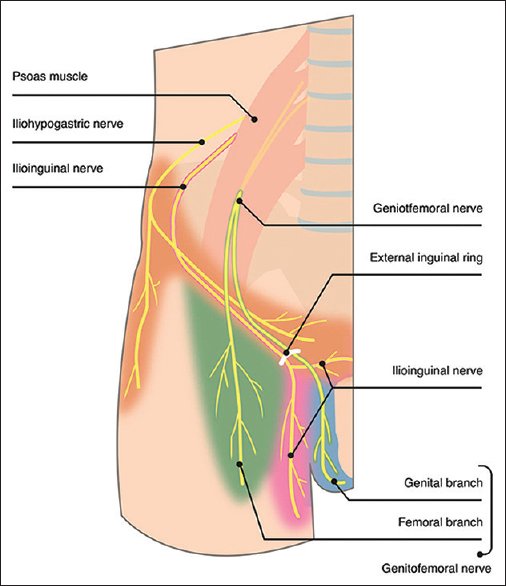
– Referred pain from myofascial structures in the deep hip flexors, especially if involving some peripheral compression of the anterior peripheral nerves that exit that those levels: the femoral nerve, the ilio inguinal nerve, and the lateral femoral continues nerve. This pain can be really tricky to assess, since it will not readily show up on advanced imaging like MRI. During physical examination, deep lateral palpation of those structures can usually be pretty revealing, and the fact that very often activities involving hip flexion can be very triggering.
– The hip joint, or more precisely the acetabular femoral joint (AF joint) . This is the ball and socket joint between the socket in the pelvis (acetabulum) , and the femoral head. This is not usually a joint that is subject to primary misalignments due to its ball and socket nature, although it certainly can, but is subject to articular cartilage degeneration, and tearing and catching of the cartilage rim also known as the labrum. There are specific orthopedic testing that can help isolate the AF joint is the source of the problem, and in addition pain from imaging as well as advanced imaging like MRI can be very diagnostic of the problem starting in that structure. From a history standpoint, patient will often report the sensation of catching or clicking, and pain triggered by hip movement rather than lumbar movement.
– The sacroiliac joint. The sacroiliac is a rather large vertical/horizontal articulation at the base of the sacrum, and the anterior portion of the sacroiliac joint can refer pain to the groin. This would happen with misalignment of the sacroiliac joint internally, that will be often associated with deep pain in the buttocks, difficulty with flexibility in the affected side of the pelvis, and standing with a toe out position on the affected side.
So groin pain can come from many different sources, but it should not be a mystery and a good physical examination can usually point the patient and the treating doctor into the right direction.